


This article considers a number of recent medical developments in relation to COVID-19 and the implications of the new vaccine for Northern Ireland.
Coronaviruses are viruses that cause respiratory infections. COVID-19 is a highly infectious disease caused by a novel form of coronavirus – known as severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). Once the virus has entered the cells of the body, the viral spikes on the surface can bind to host cells, replicate many times and go on to infect other cells. The body triggers an immune response to fight the virus. Although most people who contract the disease have mild to moderate symptoms, for those with severe disease, it can lead to pneumonia, organ failure, and death.
COVID-19 was first reported in December 2019 and has since been declared a global pandemic. One year on, and over 71 million cases and 1.6 million deaths worldwide have been reported. These are likely to be considerable underestimations of the true number of COVID-19 cases and deaths. The nature of the virus has forced most countries around the world to lockdown or restrict their citizens’ movements to protect life and reduce pressure on hospital systems. The disruption and repercussions of the virus has led to devastating and long-lasting impacts on people, their livelihoods, and the global economy.
Transmission
Transmission of COVID-19 primarily occurs through respiratory droplets generated by breathing, coughing, talking and sneezing from an infected person who is in close contact with others. Droplets can also be transmitted via contact with contaminated surfaces.
Difficulties in detecting COVID-19 and its transmission are compounded because it can spread, as if by stealth, in people who have no symptoms (asymptomatic), and those not yet presenting with symptoms. Asymptomatic carriers may never know they have had the virus; they may never have been tested and thus, could spread it unwittingly. Given the absence of population-wide antibody testing, there is no true indication of how many people are asymptomatic. Different studies suggest rates between 5% to 80%.
In addition, for reasons that are still poorly understood, re-infections can occur, indicating that immunity against the virus may wane. Whether a past infection will prevent a more severe infection if re-exposure occurs is not known at present.
Public health advice has recommended several protective measures like regular hand washing, social distancing, face coverings in certain circumstances, and early quarantine to control viral spread.
Risk factors
Increasing age and male gender are significant risk factors for severe infection of COVID-19. Key at risk groups include residents of care homes, healthcare workers, Black, Asian and Minority Ethnic groups and some people with underlying health conditions, such as asthma, cancer, obesity, lung disease and diabetes. Evidence also suggests that health inequalities contribute to higher rates of mortality and poorer health outcomes from COVID-19 in low income families and more deprived communities.
Children
Fewer cases of COVID-19 have been reported in children when compared with adults (up to 5% of cases). According to the Royal College of Paediatrics and Child Health, young children infected with COVID-19 transmit it less readily than adults and are less likely to develop severe symptoms. Research suggests hospitalisation rates in children are low, as is mortality. Data also suggests that children with certain underlying medical conditions might be at increased risk of developing severe illness. Children can also be asymptomatic, and teenagers are believed to be more likely to transmit the virus than younger children. There has also been the emergence of a rare but serious inflammatory syndrome (similar to Kawasaki disease), known as PIMS, noted in some children previously thought to have been infected with COVID-19.
Long term side effects
There have also been noticeable cases of people who had COVID-19 (either mild or severe) experiencing adverse health effects for some time after infection. This has been termed ‘Long Covid’. Evidence suggests that Long Covid may be several distinct syndromes. Symptoms can include respiratory or cardiovascular issues, mental health problems, inflammation, a protracted loss of taste and smell, gastrointestinal problems, headaches, and fatigue to name a few. Currently new clinical guidance and patient pathways are being developed to treat such cases and more robust research is needed to understand and manage the long-term health consequences of COVID-19.
The picture in Northern Ireland
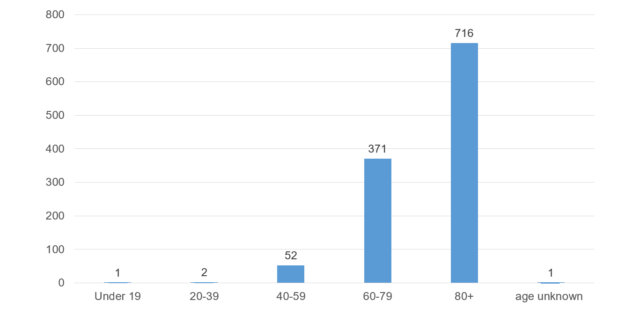
Nearly one year on since the virus was first discovered, almost 1 million tests for COVID-19 have been administered in Northern Ireland and over 55,000 positive cases confirmed. At the time of writing,1,143 deaths have been reported by the Department of Health (Northern Ireland) as a direct or contributing factor to the cause of death from COVID-19. These are broken down by age group in Chart 1. As can be seen, the highest number of deaths have occurred in the over 80 age group. Three deaths have been reported in people under 40 years of age. At the time of writing, there have been 590 male deaths and 552 female deaths reported (the age and gender of one patient was not reported). Belfast has experienced the highest number of deaths (275).

What are the potential solutions being investigated?
There is no cure for COVID-19 at present. Nevertheless, research is evolving at an unprecedented rate as scientists urgently try to understand and search for effective ways to control the disease and reduce mortality and morbidity. Extensive collaborative efforts between governments, academia and industry have gone into finding suitable medical treatments.
Therapeutic interventions
A detailed overview of the latest therapeutics being trialed is available here. Treatment options undergoing investigation include repurposing existing medications and the creation of new medical treatments as described in more detail below.
Some antiviral drugs such as Remdesivir, have been trialed to see if they can stop the virus replicating. Research has shown Remdesivir can improve recovery time in some hospitalised patients, but not others. Although it has been approved for use in certain circumstances by some jurisdictions – including the UK and USA, the World Health Organisation (WHO) has recently issued a recommendation against its use in hospitalised patients. This follows the lack of evidence to support its use, based on results from the WHO’s international SOLIDARITY trial. Other medicines like Lopinavir-Ritonavir used for HIV, and hydroxychloroquine, the anti-malarial drug, have been deemed not effective in treating COVID-19 patients – according to the UKs RECOVERY Trial which is one of the world’s largest randomised trials of COVID-19 treatments. Some of these drugs are now being trialed at different stages of the disease to see if they are effective.
Corticosteroids (anti-inflammatories) such as dexamethasone and hydrocortisone are also being examined to ascertain their effects on organ dysfunction and lung injury, resulting from inflammation from COVID-19. Low dose dexamethasone has been proven effective in reducing death in up to one third of ventilated patients with severe COVID-19. But evidence indicates that it does not appear to help those with milder symptoms. Trials for other arthritic anti-inflammatory medications like Baricitinib and Tocilizumab are also being investigated and the anti-inflammatory Colchicine has also recently been incorporated in the RECOVERY Trial.
Trials for blood derived products such as convalescent plasma – collected from patient donors who have recovered from COVID-19 – are also underway. Plasma may contain antibodies that the patient’s immune system has produced whilst fighting the virus. These antibodies are then transfused into patients whose immune systems are struggling to develop them. A recent review of evidence by Cochrane states that it is not clear if this type of treatment may be of benefit for COVID-19 patients. The safety and efficacy of these transfusions requires more robust clinical data. Two major convalescent plasma trials are currently underway in the UK.
Monoclonal antibody therapies used to treat autoimmune diseases like rheumatoid arthritis and cancer are also being explored. Rather than having chemical compounds, they are based on natural antibodies; proteins the body produces to defend itself against disease. These are created in the laboratory to primarily target the protein spikes which protrude on the surface of the virus, to block its ability to attach and infect human cells. Some examples include Regeneron’s “antibody cocktail” REGN-COV2 which contains two monoclonal antibodies. The rationale for double therapy is to reduce the chances for the virus to develop resistance to both parts of the drug. Data from Regeneron states it has been successful in the outpatient setting at reducing the viral levels in mild to moderate COVID-19 patients at risk of poor outcomes. Another monoclonal therapy under investigation is Bamlanivimab, produced by Eli Lilly. Despite showing some positive outcomes in decreasing hospitalisation and patients’ viral load compared to the placebo group, there is insufficient data at present to recommend either for or against its use in the treatment of outpatients with mild to moderate COVID-19. Both REGN-COV2 and Bamlanivimab have been given emergency use authorisation in the USA for non-hosptialised patients.
The race for a vaccine
A recent article published in the Lancet suggests that vaccination is widely regarded as the only true exit strategy from the current pandemic. As a key part of preventative medicine, the NHS describes vaccines as “the most effective way to prevent infectious diseases.”
In the UK, the routine immunisation schedule provides protection against a range of vaccine-preventable infections, including measles, meningococcal infections and human papillomavirus (HPV). There are also vaccinations for seasonal illness like flu and shingles. Vaccinations are not mandatory in the UK.
Vaccines are designed to prevent diseases by harnessing the natural activity of the immune system. When germs, such as bacteria or viruses, invade the body, they attack and multiply and this can lead to infection and illness. The immune system uses several tools to fight infection. After the infection, the immune system remembers what it has learned about protecting the body. Vaccines work in a similar way – by imitating an infection and causing the immune system to respond before a person experiences symptoms of the disease.
Types of vaccines in development
In January 2020, the genetic sequence of SARS-CoV-2 (COVID-19) was published. An intense global effort ensued to accelerate vaccine development. Several broad classes of potential vaccines for COVID-19 are in development as shown below:
| Inactivated or weakened virus vaccines | These use a form of the virus that has been inactivated or weakened so it does not cause disease, but still generates an immune response. |
| Protein-based vaccines | These use harmless fragments of proteins or protein shells that mimic the COVID-19 virus to generate an immune response. |
| Viral vector vaccines (adenoviral) | This type of vaccine uses a genetically engineered virus so that it cannot cause disease, but produces coronavirus proteins to generate an immune response. |
| RNA and DNA vaccines | These are cutting-edge approaches that use genetically engineered RNA or DNA to generate a protein that prompts an immune response. |
It is understood that a range of vaccines will need to be developed and produced at scale to tackle COVID-19 world-wide and meet the global demand. WHO data shows that over 200 COVID-19 vaccine candidates are being developed; 52 candidate vaccines are currently undergoing clinical testing, and at least another 162 candidates are at preclinical stages.
The process of vaccine development usually takes many years and not all vaccines will be successful. Development involves a number of phases, including large numbers of human clinical trials. As highlighted in this recent article in The Lancet, assessing the clinical efficacy of a vaccine for COVID-19 is extremely challenging.
Understandably, the public have also voiced concerns over how rigorously and extensively the vaccines will be tested, given the pace at which they have been developed. Experts have stated that due to the urgency of the pandemic, rather than trials being conducted sequentially over time, different stages of trials have been conducted in parallel without compromising on safety measures. This has allowed faster data collection and ongoing (rolling) reviews that give regulators access to data as it becomes available.
There have also been challenges with misinformation about COVID-19 vaccines which could lead to a reduction in vaccine uptake levels. The British Medical Association has published a report aimed at improving immunisation levels in the UK. It suggests that raising public awareness and understanding of immunisation programmes is key. There have also been requests, as described here, for more transparency over vaccine data to enable public trust and confidence to be built.
What COVID-19 vaccines could be administered in the UK?
The UK’s Joint Committee on Vaccination and Immunisation (JCVI) has stated that the first priorities for any COVID-19 vaccination programme should be the prevention of COVID-19 mortality and the protection of health and social care staff and systems. It also states that in order to interrupt transmission of COVID-19:
…mathematical modelling indicates that we would need to vaccinate a large proportion of the population with a vaccine which is highly effective at preventing infection (transmission).
In May 2020, a Vaccines Taskforce was set up in the UK under the Department for Business, Energy and Industrial Strategy. Its purpose is to ensure that the UK has rapid access to clinically effective and safe vaccines. A report by the National Audit Office shows significant investment has been made by the UK Government in terms of planning and development of potential vaccines.
An overview of the regulatory processes involved in licensing COVID-19 vaccines can be found in this UK Parliament paper. Before a vaccine is approved in the UK, the regulatory authority – Medicines and Healthcare products Regulatory Agency (MHRA) – rigorously reviews the safety, quality and effectiveness from the trial data. The MHRA also seeks advice from the Commission on Human Medicines to critically assess the data before advising government on the use of any potential vaccine. Importantly, once licensed, the safety of the vaccines are monitored on an ongoing basis.
Given the uncertainty about which vaccines may be found to be safe and effective, the UK Government’s approach was to increase vaccine options if some do not receive regulatory approval. In November 2020, the Government announced it had secured “357 million vaccine doses from 7 different developers, giving the UK the best possible chance of protecting the public from coronavirus as soon as possible.”
The vaccines that could be administered if proven safe and effective are presented in Table 1. Many are in the late stages of clinical trials:
| Vaccine developer and quantities secured | Class of vaccine |
| 100 million doses of Uni of Oxford/ AstraZeneca vaccine | adenoviral |
| 40 million doses of BioNTech/Pfizer vaccine | mRNA |
| 7 million doses of Moderna vaccine | mRNA |
| 60 million doses of Novavax vaccine | protein adjuvant |
| 60 million doses of Valneva vaccine | inactivated whole virus |
| 60 million doses of GSK/Sanofi Pasteur | protein adjuvant |
| 30 million doses of Janssen vaccine | adenoviral |
Table 1: COVID-19 vaccines and doses currently secured for the UK
First vaccine approval in the UK: Pfizer/BioNTech
On 2 December 2020, the MHRA announced that it had approved an Emergency Use Authorisation for the Pfizer/BioNTech COVID-19 vaccine (BNT162b2). This is not a live virus. The active ingredient is messenger RNA (mRNA) which carries instructions for making the virus’s spike protein, used to gain entry to cells.
The results of the Pfizer/BioNTech vaccine trials included over 43,000 participants. Half of those participating received the vaccine, the other half a placebo. Two doses of the vaccine were given, 21 days apart. In total, 170 people became ill with COVID-19; 8 from the vaccine group and 162 from the placebo group. The data indicates high efficacy in all age groups (16 years and over). In terms of safety, adverse events in those who received the vaccine were 0.6%, compared to 0.5% in the placebo group. The study demonstrated an efficacy rate of 95% seven days after the second dose, indicating that those who receive the vaccine should be protected from becoming seriously ill with COVID-19.
This is the first time an mRNA vaccine has been licensed and rolled out at scale. However, some features of the vaccine have logistical implications in terms of deployment. For example, this particular vaccine requires storage at ultra-low temperatures (-70C), it has a 5 day shelf life when defrosted, and at present, batches of the virus cannot be split into smaller packs – each batch contains 975 doses.
In the months ahead, it is likely that more vaccines will become available if the associated clinical trial data is deemed to be safe and effective.
What does a vaccine mean for Northern Ireland?
On 3 December 2020 Health Minister Robin Swann MLA and two Department of Health officials briefed the Northern Ireland Assembly’s Committee for Health that the Pfizer/BioNTech COVID-19 vaccine would be rolled out locally on a phased basis as it becomes available. Health officials also stated that vaccines will be administered by priority groups, as advised by the JCVI. The JCVI priority list is as follows:
| Group 1 | Residents in a care home for older adults and their carers. |
| Group 2 | All those 80 years of age and over, together with frontline health and social care workers. |
| Group 3 | All those 75 years of age and over |
| Group 4 | All those 70 years of age and over, together with clinically extremely vulnerable individuals. Clinically extremely vulnerable individuals include, among others, transplant recipients, some cancer patients and people on immunosuppression therapies. |
| Group 5 | All those 65 years of age and over |
| Group 6 | All individuals aged 16 years to 64 years with underlying health conditions which put them at higher risk of serious disease and mortality. These include, among others, chronic respiratory and heart disease, morbid obesity, diabetes and severe mental illness. |
| Group 7 | All those 60 years of age and over |
| Group 8 | All those 55 years of age and over |
| Group 9 | All those 50 years of age and over |
Roll out in Northern Ireland will be delivered in 5 phases starting with Phase 1 – those listed in Priority Groups 1 and 2 in December 2020. Officials envisage that by Phase 3 of the plan, all priority groups listed above will have been offered the vaccine (around spring 2021). Between spring and summer 2021, mass vaccination for those not in the priority groups who are eligible will be underway. Vaccines will be given on a voluntary basis if there is informed consent (or by a responsible person for those who lack capacity). Health officials have stated they aim to have a vaccine uptake rate of around 75% (over 1.4 million people).
The first vaccines administered
On 8 December 2020, some medical staff and care home residents in Northern Ireland received the first dose of the Pfizer/BioNTech COVID-19 vaccine.
Conclusion
COVID-19 is the biggest global health challenge of our time. As treatments continue to be developed and tested, it is likely we will have to live with the disease for some time to come. Many questions remain unanswered about the virus. Yet it is hoped that a vaccine programme will help reduce transmission and disease, albeit that immunity will take time to build in the population. In the meantime, Department of Health advice is for everyone to keep adhering to social distancing guidance.